
Introduction
Shoulder pathologies
The shoulder is the most mobile joint of the human body. Rotator cuff tears, adhesive capsulitis, instability and glenohumeral osteoarthritis are the most frequent surgical indications.
Techniques
Surgical and conservative techniques
Anatomic and reverse replacements, arthroscopic cuff repairs, capsular stabilisations, ultrasound-guided infiltrations.
Shoulder anatomy
The shoulder is formed by the humerus, clavicle and scapula, which together create a spherical socket that receives the upper arm bone. The entire structure is wrapped in cartilaginous tissue that ensures fluid movement. Dislocations and minor trauma compromise the internal tissue, destabilising the joint. Shoulder orthopedic surgery has developed minimally invasive techniques over recent decades, enabling rapid functional recovery even in relatively young patients.

Anatomic and reverse shoulder replacement
Shoulder prostheses implanted by Prof. Colao's team are ultra-anatomical with low invasive impact: maximum bone preservation, minimal musculotendinous damage, very limited blood loss. The anatomic prosthesis is used when the rotator cuff is intact; the reverse prosthesis when the cuff is completely damaged and the joint system must be redesigned. Within 24 hours the patient can begin meaningful rehabilitation: many patients return to tennis and full rotation movements without restriction.

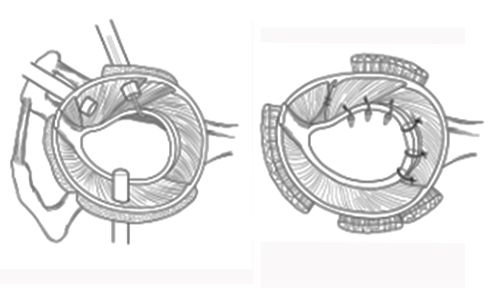
Rotator cuff repair
Rotator cuff repair procedures are performed with microsurgical techniques through a mini subacromial approach, ensuring rapid shoulder mobility recovery without motor limitations. Post-operative physiotherapy has minimal duration. The limited access reduces trauma to surrounding tissues and accelerates healing, allowing patients to recover full joint function in previously unthinkable timeframes.
Recurrent shoulder dislocation
Recurrent shoulder dislocation causes patients to restrict use of the arm for fear of the joint slipping out. Prof. Colao's arthroscopic soft-tissue repair procedures have minimal impact and consistently reduced rehabilitation times. After a period of immobilisation with a brace (ultrasling at 15° abduction for 4 weeks), the shoulder recovers full stability: driving is permitted at 10 weeks, competitive sport at 4 months.

Clinical information
Shoulder replacement
- Procedure
- Ultra-anatomical total shoulder replacement (anatomic or reverse), low invasive impact
- Hospital stay
- Approximately 3 days
- Anaesthesia
- Regional, general or combined anaesthesia
- Post-op course
- Active rehabilitation from 24 hours post-op; 4-6 weeks of physiotherapy
- Rehabilitation
- Check-ups at 1, 3 and 6 months; full recovery of work and sporting activity
Rotator cuff repair
- Procedure
- Microsurgical repair via mini subacromial approach
- Hospital stay
- Approximately 3 days
- Anaesthesia
- Regional, general or combined anaesthesia
- Post-op course
- Joint function restored within hours; short-duration physiotherapy
- Rehabilitation
- Check-ups at 1, 3 and 6 months; progressive cuff strengthening exercises
Recurrent shoulder dislocation
- Procedure
- Arthroscopy with capsulo-ligamentous repair
- Hospital stay
- Day hospital
- Anaesthesia
- General anaesthesia
- Post-op course
- Ultrasling brace at 15° for 4 weeks; driving permitted at 10 weeks
- Rehabilitation
- 4-6 weeks of rehabilitation after brace removal; competitive sport at 4 months
The information has educational value and does not replace specialist medical examination.
Book a visit